Inspirational journeys
Follow the stories of academics and their research expeditions
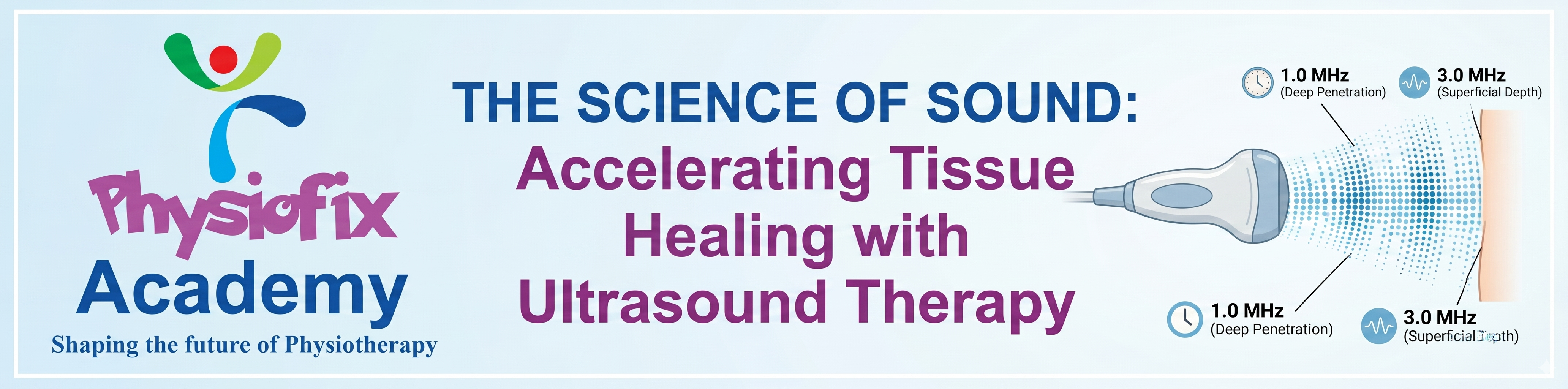
From Cavitation to Collagen: Understanding the Physical Principles of Therapeutic Ultrasound

Principles & Biophysical Mechanisms: How It Works
Therapeutic ultrasound operates by converting electrical energy into high-frequency acoustic energy via the reverse piezoelectric effect. This process occurs inside an applicator head containing a synthetic ceramic crystal (such as lead zirconate titanate) that expands and contracts in response to an alternating electrical current.
These rapid crystal oscillations generate longitudinal sound waves that travel into biological tissue, alternating between phases of high pressure (compression) and low pressure (rarefaction) (Miller et al., 2012).
Key Parameters:
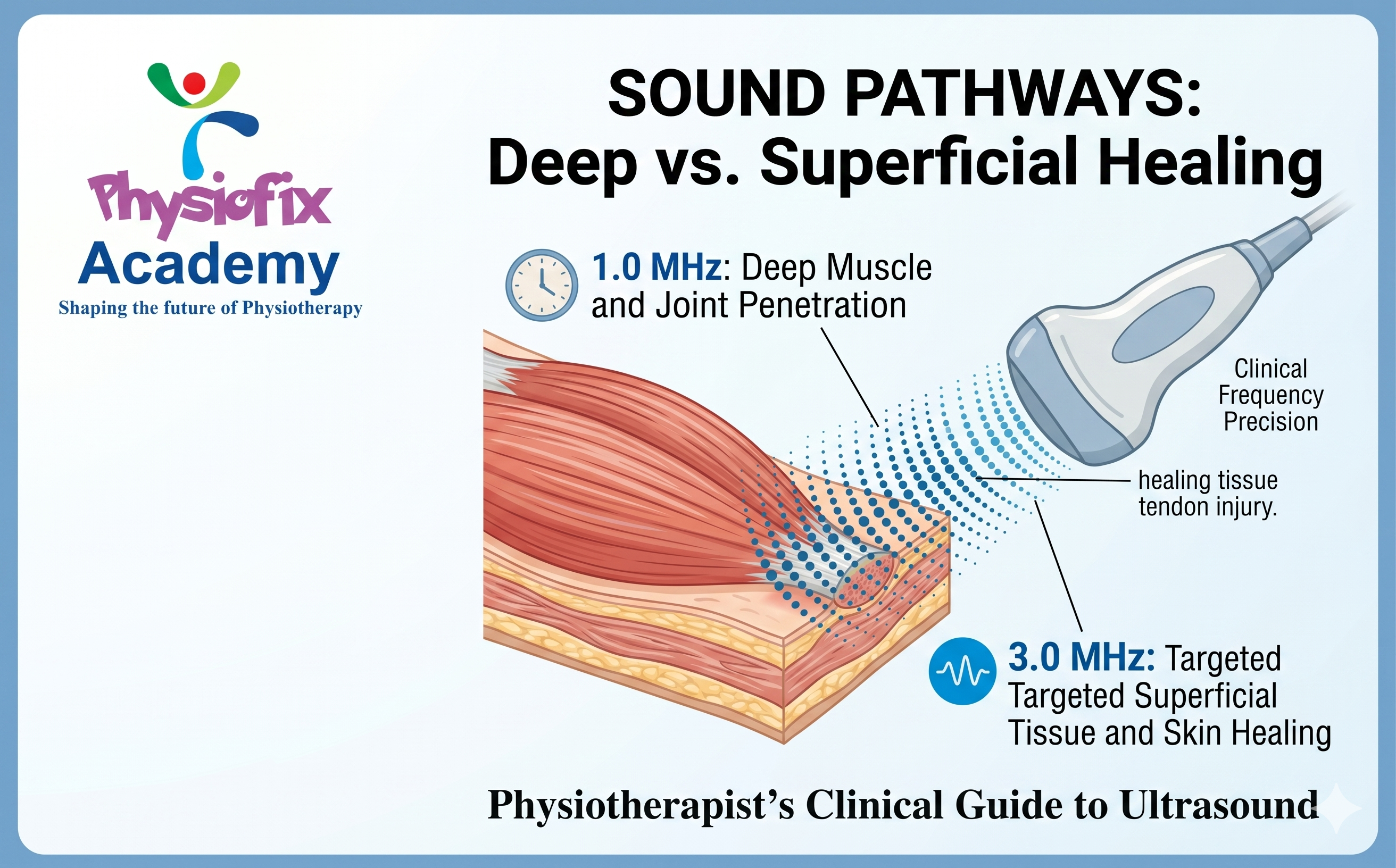
Frequency: Determines the depth of penetration. A frequency of 1.0 MHz penetrates deeply (up to 5 cm to target deep muscles and joint capsules), while 3.0 MHz is absorbed superficially (up to 1.5 cm to target skin, superficial tendons, and fascia) (Bader et al., 2024).
Waveform Mode: Dictates whether energy delivery is uninterrupted (Continuous Mode) to generate thermal accumulation, or interrupted (Pulsed Mode) to favor purely mechanical, non-thermal effects.
History & Adoption in Physical Therapy
The transition of ultrasound from industrial use to clinical medicine followed a clear timeline:
1930s–1940s (Early Exploration): Medical researchers began experimenting with ultrasound's biological effects, primarily focusing on intense tissue heating and localized, highly destructive interventions in the brain (such as treating Parkinson's disease by creating targeted lesions) (ter Haar & Coussios, 2007; Miller et al., 2012).
1950s (The Pivot to Low-Power): Rather than destroying tissue, researchers developed low-power applications (around $1.0\text{ MHz}$) specifically designed to manage inflammatory musculoskeletal conditions like tendinitis or bursitis safely (Miller et al., 2012).
1970s (Widespread Physical Therapy Adoption): Ultrasound became a standard electrophysical agent in physical therapy clinics worldwide for pain relief and soft tissue restoration (Robertson & Baker, 2001; Miller et al., 2012).
Modern Era (Expanded Scope): Beyond standard therapeutic heating and cellular repair, contemporary physical therapists also utilize Point-of-Care Ultrasound (POCUS) for rehabilitative muscle morphology imaging, diagnostic tendinopathy screens, and guiding dry-needling procedures (Whittaker et al., 2019).
Physiological Effects on Tissue
The biological responses triggered by therapeutic ultrasound are divided into thermal and non-thermal categories:
Thermal Effects (Continuous Mode)
When ultrasound waves pass through tissue, friction between vibrating molecules converts acoustic energy into heat (Miller et al., 2012). Tissues rich in collagen—such as tendons, ligaments, joint capsules, and fascia—have high absorption coefficients and heat rapidly (de Jesus et al., 2019). Clinical outcomes include:
Accelerated local metabolic rate and enhanced blood flow.
Increased collagen extensibility, which improves range of motion when combined with stretching.
Altered nerve conduction velocities, providing temporary pain relief and reducing muscle spasms (Bader et al., 2024).
Non-Thermal Effects (Pulsed Mode)
Non-thermal responses occur regardless of thermal accumulation and are driven by two main physical processes:
Cavitation: The formation, growth, and pulsation of microscopic gas bubbles within extracellular fluid due to pressure changes (Miller et al., 2012). Stable cavitation alters cell membrane permeability without destroying tissue.
Acoustic Streaming / Micro-streaming: The localized, one-directional movement of fluids around these pulsating bubbles and cell membranes (Bader et al., 2024).
This mechanical stress deforms cell membranes, opening calcium channels and stimulating cellular activity. This activity accelerates the degranulation of mast cells, enhances macrophage performance, and boosts fibroblast synthesis of collagen to accelerate tissue repair (Miller et al., 2012).
The Science of Dosimetry Calculations
To achieve reproducible therapeutic effects, clinicians must transition away from arbitrary "10-minute treatments" and calculate specific energy profiles. Therapeutic ultrasound dosing relies heavily on three key variables: the Effective Radiation Area (ERA), the Beam Non-uniformity Ratio (BNR), and Total Cumulative Energy (de Jesus et al., 2019).
CORE DOSIMETRY FORMULAS
Transitioning from a Passive Adjunct to an Active Monotherapy
Historically, ultrasound has faced criticism regarding its standalone efficacy because it is frequently used as a passive, unmeasured "add-on" at the end of a session (Robertson & Baker, 2001). To use ultrasound as an active, effective clinical tool, practitioners must treat it as a targeted primer for mechanotransduction rather than a passive modality.
1. The Therapeutic Window Strategy
Thermal ultrasound increases tissue elasticity for only 5–10 minutes post-application before tissue temperature cools back to baseline.
The Adjunct Pitfall: Applying ultrasound, wiping off the gel, and sending the patient home.
The Monotherapy Strategy: Administer continuous thermal ultrasound immediately before or simultaneously with manual joint mobilizations, dynamic stretching, and eccentric loading exercises to structurally re-align newly pliable collagen fibers.
2. Matching Modality to Tissue Stage
Therapists must align the parameter selection with the specific phase of tissue healing rather than applying a generic setting:
[Acute Phase] --> Pulsed Mode (20%) --> Non-Thermal / Cellular Permeability
[Subacute Phase] --> Pulsed Mode (50%) --> Transition Phase / Controlled Mechanics
[Chronic Phase] --> Continuous Mode (100%)--> Deep Tissue Heating / Collagen Extensibility
3. Precise Boundary Maintenance
Because air reflects nearly 100% of acoustic energy, maintaining an optimal acoustic interface is critical. Therapists must use sufficient conductive gel, keep the transducer perfectly perpendicular to the skin, and move the soundhead at a slow, deliberate speed (approx 4/s) strictly within an area no larger than 2 to 3 times the ERA (de Jesus et al., 2019). This approach avoids under-dosing and ensures that the target tissue receives the exact calculated energy density required to stimulate structural adaptation.
References
Bader, K. B., Padilla, F., Haworth, K. J., Ellens, N., Dalecki, D., Miller, Douglas L., & Wear, K. A. (2024). Overview of Therapeutic Ultrasound Applications and Safety Considerations: 2024 Update. Journal of Ultrasound in Medicine, 44(2), 381–433.
Cited by: 47
de Jesus, J. F., de Albuquerque, T. A. B., Shimba, L. Girardi, Bryk, F. F., Cook, J., & Pinfildi, C. E. (2019). High-energy dose of therapeutic ultrasound in the treatment of patellar tendinopathy: protocol of a randomized placebo-controlled clinical trial. BMC Musculoskeletal Disorders, 20(1).
Miller, Douglas L., Smith, N. B., Bailey, M. R., Czarnota, G. J., Hynynen, K., & Makin, I. R. S. (2012). Overview of Therapeutic Ultrasound Applications and Safety Considerations. Journal of Ultrasound in Medicine, 31(4), 623–634.
Cited by: 1001
Robertson, V. J., & Baker, K. G. (2001). A Review of Therapeutic Ultrasound: Effectiveness Studies. Physical Therapy, 81(7), 1339–1350.
Cited by: 745
ter Haar, G., & Coussios, C. (2007). High intensity focused ultrasound: Physical principles and devices. International Journal of Hyperthermia, 23(2), 89–104.
Cited by: 1076
Whittaker, J. L., Ellis, R., Hodges, P. W., O'Sullivan, C., Hides, J., Fernandez-Carnero, S., Arias-Buria, J. L., Teyhen, D. S., & Stokes, M. J. (2019). Imaging with ultrasound in physical therapy: What is the PT’s scope of practice? A competency-based educational model and training recommendations. British Journal of Sports Medicine, 53(23), 1447–1453.
Cited by: 160
Tags:
Ultrasound Therapy Physiotherapy Tissue Healing Musculoskeletal Pain Piezoelectric Effect Cavitation Acoustic Streaming Tendonitis Knee Osteoarthritis Frozen Shoulder Soft Tissue Injury Chronic Inflammation Collagen Synthesis Fibroblast Proliferation Thermal Effects Non-thermal Effects Pulsed Ultrasound LIPUS Transducer Coupling Gel0 Comments
Categories
- Clinical Decision Making 3
- Manual Therapy 2
- Fix Your Posture, Fix Your Life: How Physiofix Helps You Stand Tall Again 1
- Therapeutic Modalities 1
Recent posts
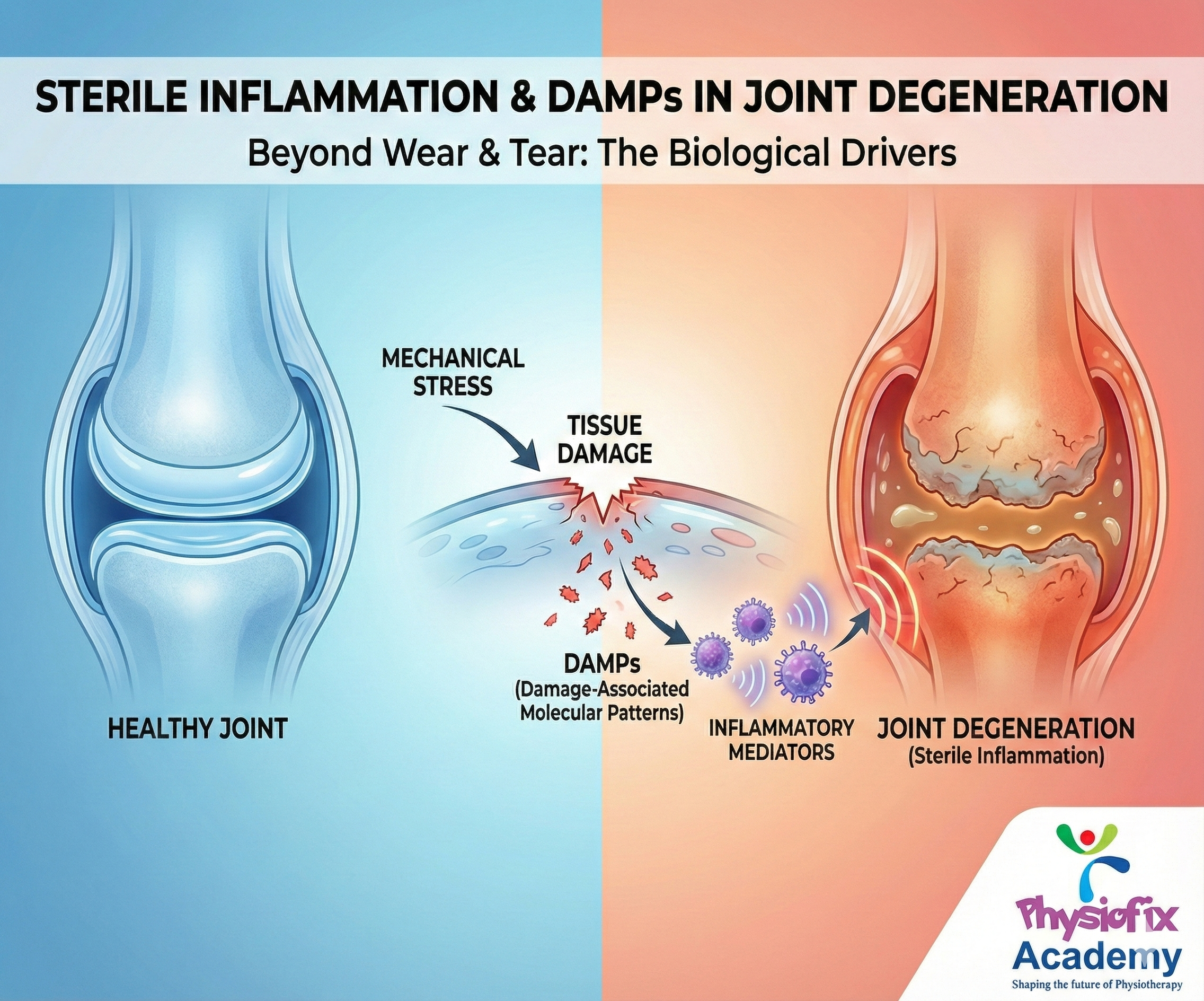
Sterile Inflammation and the Role of DAMPs in Joint Degeneration
Sun, 08 Feb 2026
Dry Needling - How to Use it
Tue, 06 Jan 2026
Leave a comment